Please note: This questionnaire is for those 14 years old or older.
If you would like to tell us more about your symptoms, please write about them in the Comment Section at the end of the Questionnaire. We will combine this information with the responses you gave in the Questionnaire to provide you with a more detailed interpretation of the results.
Directions: For each of the following questions, please check the answer that best describes your situation. If you wear glasses or contact lenses, answer the questions assuming that you are wearing them. Please answer every question.
Never = Never
Seldom = Less than 1 time / month
Occasionally = Less than 1 time / week
Frequently = At least 1 time / week
Always = Everyday
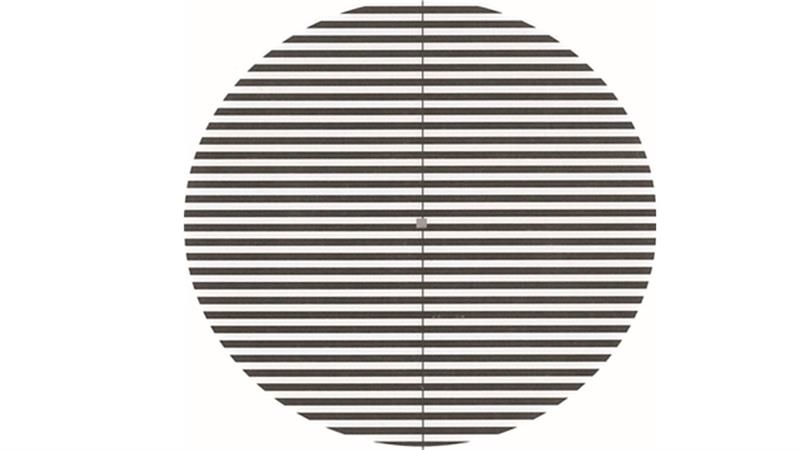
The Pattern Glare Test
The following image with the black and white stripes is called a pattern glare test. It was designed to assess the severity of a patient post-concussion or epileptic patients.
If you find this image causes a high level of discomfort to the point that you cannot look at it, this can be an indicator of a visual problem.